Abstract
State-of-the-art medical multi-modal LLMs (med-MLLMs), such as LLaVA-Med and BioMedGPT, primarily depend on scaling model size and data volume, with training driven largely by autoregressive objectives. However, we reveal that this approach can lead to weak vision-language alignment, making these models overly dependent on costly instruction-following data. To address this, we introduce ExGra-Med, a novel multi-graph alignment framework that jointly aligns images, instruction responses, and extended captions in the latent space, advancing semantic grounding and cross-modal coherence. To scale to large LLMs (e.g., LLaMa-7B), we develop an efficient end-to-end training scheme using black-box gradient estimation, enabling fast and scalable optimization. Empirically, ExGra-Med matches LLaVA-Med’s performance using just 10% of pre-training data, achieving a 20.13% gain on VQA-RAD and approaching full-data performance. In addition, it exceeds other SOTA med-MLLMs in Med-VQA benchmarks, promising a new way to integrate vision and language in medical AI. We release our checkpoints at this Github.
1 Introduction
Multi-Modal Large Language Models (MLLMs) are a range of neural network architectures that can process different types of input data, such as images, text, and audio. One important step of training MLLM is the curation of instruction-following (IF) data (Lou et al., 2023), in which a model is asked to give answers to questions in a multi-turn conversation based on a given image. This step is also implemented in the medical domain, where IF datasets encompassing medical images, clinical notes, and diagnostic data are curated (Xie et al., 2024). One example is the work of LLAVA-Med (Li et al., 2024), which leverages GPT-4 to curate 600K biomedical image-text pairs and 60K multi-modal IF data from PMC-15M (Zhang et al., 2023c). Other works follow this practice, which either scale up the amount of medical data (Xie et al., 2024; Zhang et al., 2023a; He et al., 2024) or the model size (Wu et al., 2023; Jiang et al., 2024), while the autoregressive objective loss stays the same. This practice is indeed helpful, enabling models to achieve promising performance. For example, Biomed-GPT (Zhang et al., 2023a) is excellent with multiple biomedical modalities, while MedFlamingo (Moor et al., 2023) also reports good performance on few-shot learning for medical visual question answering. However, the reliance of performance on scale poses some serious questions, especially in the biomedical domain, where IF data is scarce.
In our work, we study the effectiveness of this approach and reveal that autoregressive learning is highly data-hungry, which leads to the degradation of the performance of the model if there is insufficient IF data. To demonstrate this, we pre-train LLAVA-Med using only 10% of the original data and compare it to a version trained on the full dataset. Both models are then fine-tuned on the VQA-RAD dataset (Lau et al., 2018). As illustrated in Figure 1, despite being updated with downstream task data, performance declines sharply from 72.64% to 52.39% on VQA-RAD. This underscores the instability of medical MLLMs trained with autoregressive methods and highlights their heavy reliance on extensive medical instruction-following data to achieve satisfactory performance.
To overcome the limitations of autoregressive training in settings with limited instruction-following data, we introduce ExGra-Med, a novel multi-graph alignment framework designed to enhance cross-modal understanding in multi-modal large language models (MLLMs). Central to our method is the construction of three modality-specific graphs: one capturing visual features from a vision encoder, and two representing different textual forms of the instruction. These graphs encode semantic relationships within and across modalities, and we cast their alignment as a combinatorial multi-graph matching problem. This enables the model to learn consistent triplet-level associations among the image, the original instruction, and a semantically enriched variant. We jointly optimize this alignment objective alongside the standard autoregressive language modeling loss, thereby improving the model’s semantic comprehension, coherence, and instruction-following capabilities. To generate the enriched instruction, we employ a frozen LLM (GPT-4 (Achiam et al., 2023)) to produce a contextually extended version that preserves the original intent while emphasizing key concept relationships. The vision encoder and language model (LLaMa (Touvron et al., 2023)) independently process the image, instruction, and extension to produce node embeddings used in the alignment. Unlike simple data augmentation, our GPT-4-driven supervision introduces meaningful semantic structure, enabling fine-grained graph-based correspondence learning across modalities (Figure 2).
Our method differentiates itself from existing multi-modal alignment techniques for LLM (Park et al., 2024; Li et al., 2023a; Chen et al., 2023) in different perspectives. First, while prior contrastive objectives primarily focus on learning projections based on multi-layer perceptron (MLP) layer (Liu et al., 2024a; Chen et al., 2023) or adapters (Zhang et al., 2024; Huang et al., 2023; Alayrac et al., 2022; Li et al., 2023a) to connect frozen vision encoders with frozen language models, our algorithm directly trains LLM using the multi-graph framework.
Second, we unify and generalize pre-training algorithms commonly applied for vision-language models using pairwise contrastive learning between image-text pairs (Liu et al., 2023; Zhai et al., 2023; Khan and Fu, 2023), optimal transport (Chen et al., 2022; Nguyen et al., 2024a), or impose clustering constraints (Park et al., 2024) by integrating combinatorial formulation across cross-domain graphs. This allows us to integrate both feature and structural consistencies using graph edges, enhancing robustness for similar entities (whether images or descriptions) commonly found in medical datasets.
Finally, combinatorial graph alignment is inherently non-differentiable (Rolínek et al., 2020), and solving multi-graph alignment is computationally expensive (Pevzner, 1992). While existing approaches - such as multi-marginal optimal transport (Lin et al., 2022; Piran et al., 2024), Wasserstein barycenters (Nguyen et al., 2024b), and multi-adjacency matrix assumptions (Bernard et al., 2019; Swoboda et al., 2019) — help relax the problem, they are limited to small-scale tasks and require multiple solver steps, making them inefficient for LLM training. We overcome these challenges by leveraging modern implicit maximum likelihood estimation techniques (Niepert et al., 2021; Minervini et al., 2023). This enables efficient gradient estimation and allows for fast forward and backward propagation through large LLMs (e.g., LLaMa-7B), using a barycenter graph (Agueh and Carlier, 2011) for alignment. As a result, the model can scale effectively with extensive datasets on large LLMs while maintaining alignment performance.
In summary, we make the following key contributions:
-
•
We reveal the data-demanding nature of autoregressive modeling in pre-training medical-MLLM (LLaVa-Med), showing that insufficient instruction-following data leads to significant performance drops on downstream tasks, even after fine-tuning.
-
•
We introduce a new multi-graph alignment objective, namely ExGra-Med, that establishes triplet correlations among images, their instruction-following context, and their enriched versions. Furthermore, we developed an efficient solver for training with LLMs (LLaMa-7B) that can scale with the size of the dataset and model.
-
•
We empirically demonstrate that using a small amount of pre-training data, ExGra-Med can achieve performance comparable to LLaVa-Med trained on data. Additionally, when trained on larger datasets, ExGra-Med outperforms several state-of-the-art med-MLLMs and advanced multi-modal pre-training algorithms across three Medical VQA tasks.
2 Multi-graph Alignment Learning
We denote the vision encoder, projector and LLM by , respectively. Figure 2 presents our ExGra-Med algorithm, which learns model through triplet alignment in instruction tuning data. Before detailing each component, we provide some notations used in this paper.
Notation. Given any tensor and matrix , we use to denote the tensor-matrix multiplication, i.e., the matrix . Given , we define . Moreover, we define the matrix scalar (or inner) product associated with the Frobenius norm between two matrices and as , i.e., . We write for any natural number .
2.1 Extended context enriched medical IF data
Recent work shows that longer context improves LLMs’ instruction-following by retaining relevant information (Liu et al., 2024b; An et al., 2024; Pawar et al., 2024). To leverage this, we enrich medical instruction data with contextually extended paraphrases where both original and extended ones are used: originals preserve domain-specific precision, while extensions add semantic depth. This combination enhances image embeddings and helps the LLM generate contextually rich, consistent responses across modalities and linguistic forms.
In particular, we define instruction samples as where is an input image, a question, and an answer at round in multi-round conversation of length . In the medical domain, questions are often generic, and answers usually encapsulate the relevant information. Therefore, we focus on extending answer . Using GPT API with prompt, we generate an extended context for each as follows:
| (1) |
The details of are illustrated in the Appendix C. An example for is in Table 5. Note that other frozen LLMs such as Gemini are also valid in our method (Table 4).
2.2 Vision-Language Multi-graph Construction
We process each image by dividing it into patches with is patch size (denote is list of image patches). Then, patch features are extracted via a pre-trained ViT and projected into . The global image representation is obtained as . For each language input with , a LLM extract embeddings as , which are aggregated over conversation rounds into . Despite its simplicity, it remains an effective approach with a clear observed margin of separation between the distinct distributions (Table 4 in the Ablation study).
Given a batch of instruction samples, we construct three graphs , , and for visual features, original text embeddings, and extended context embeddings, respectively. Then, we define 3 set of nodes ; for each with corresponding node features , . The edges for afterward are constructed via k-NN algorithm on . Finally, a message-passing network is applied on three built graphs to learn richer node representations. This approach has proven effective for representation learning (Tang et al., 2022; Ju et al., 2024), resulting in aggregated feature-node matrices as , with .
2.3 Scalable Multi-graph Alignment
Our goal is to align , and to enforce a triplet constraint between image, original instruction, and extended embeddings. However, structure-aware alignment across domains () is costly. For instance, a pairwise graph alignment approach, while applying specific constraints to maintain consistency between correspondences (Bernard et al., 2019; Swoboda et al., 2019), scales impractically for large multi-modal data when increases (perform times). Instead, we leverage the barycenter concept from optimal transport (Guo et al., 2020; Altschuler and Boix-Adsera, 2022) by reformulating alignments into separate mappings with a barycenter graph. Unlike prior unsupervised methods, we directly define the barycenter using known triplet pairs across three graphs, which significantly reduces complexity and improves efficiency in LLM settings (Tab.4).
Specifically, we define a barycenter graph representing triplet pairs with a correspondence feature node as with . Edges is formed using k-NN as previous graphs. We now state the multi-graph alignment as:
| (2) |
where represents valid mappings between and , and be vertex and edge affinity tensors between and , and . The set indicates for all admissible pairs that encode a valid matching between and .
| (3) |
Due to NP-hard complexity, we use heuristic solvers utilizing Lagrange decomposition techniques (Swoboda et al., 2017; Rolínek et al., 2020).
Given and is true triplet alignments between the graph to and , to optimize feature representations such that be identical to explicitly, we minimize the Hamming loss:
| (4) |
Due to the piecewise constant nature of the graph matching objective, which poses a challenge for gradient computing, we apply IMLE techniques (Niepert et al., 2021; Minervini et al., 2023), a method permitting estimate gradients over solutions of the combinatorial optimization problem by taking the difference between solutions of matching problem perpetuated by Gumbel noise.
In particular, given and for each , we compute:
| (5) | ||||
| (6) |
3 Experiments
3.1 Med-VQA Comparison:
To highlight the strengths of ExGra-Med, we compare it with vision-language pre-training methods at 10% and 40% data scales, and benchmark it against other med-MLLMs using the full dataset.
Datasets. We test pre-trained models on three prominent biomedical VQA datasets: VQA-RAD (Lau et al., 2018), SLAKE (Liu et al., 2021), and PathVQA (He et al., 2020). All datasets include open-ended (e.g., what, why, where) and closed-ended (yes/no or two-option) question types. Statistical detail of datasets are presented in Appendix D.1.
Baselines - I) Comparing with other vision-language pre-training algorithms, we compare ExGra-Med against two categories: (1) two-modality methods and (2) multi-modal methods spanning three or more modalities.
- For two-modality methods, we include InfoNCE-based methods (Khan and Fu, 2023; Liu et al., 2023), SigLIP (Zhai et al., 2023), PLOT (Chen et al., 2022), and VLAP (Park et al., 2024). Among this, while SigLIP adapts the Sigmoid loss on image-text pairs to break the global view of the pairwise similarities for normalization, resulting in scaling in large batch size, PLOT aligns image patches with text embeddings using optimal transport, and VLAP employs assignment prediction to bridge visual-LLM modality gaps.
- For multi-modal learning (three or more modalities), we compare against PAC-S (Sarto et al., 2023), GeoCLAP (Khanal et al., 2023), and IMAGEBIND (Girdhar et al., 2023). PAC-S combines contrastive losses across modality pairs: (image–text), (image–augmented text), and (text–augmented text). GeoCLAP applies CLIP-style learning to cross-domain pairs while IMAGEBIND extends InfoNCE to unified multi-modal embeddings.
II) Comparing with other med-MLLMs, we benchmark LLaVA (Liu et al., 2024a), LLaVA-Med (Li et al., 2024), Med-Flamingo (Moor et al., 2023), Med-Dr (He et al., 2024), Biomed-GPT (Zhang et al., 2023a), M2I2 (Li et al., 2023b), GPT-4o (Achiam et al., 2023), and Med-MoE (Jiang et al., 2024). Except for LLaVA and GPT-4o, all models leverage biomedical pre-training. With exception of LLaVA, which we reproduced, baseline results are taken from literature. Additionally, we introduce ExGra-Med + DCI, integrating multi-scale vision features (Yao et al., 2024) to enhance local-global medical image understanding.
Method #Para VQA-RAD SLAKE PathVQA Overall Open Closed Avg. Open Closed Avg. Open Closed Avg. LLaVA-Med 7B 63.65 81.62 72.64 83.44 83.41 83.43 36.78 91.33 64.06 73.37 BiomedGPT-B 182M 60.9 81.3 71.1 84.3 89.9 87.1 28 88 58 72.07 M2I2 - 61.8 81.6 71.7 74.7 91.1 82.9 36.3 88 62.15 72.25 BioMed-CLIP 422M 67.6 79.8 73.7 82.5 89.7 86.1 Med-Dr 40B 37.5 78.9 58.2 74.2 83.4 78.8 33.5 90.2 61.85 66.28 LLaVA (general) 7B 50 65.1 57.55 78.2 63.2 70.7 7.7 63.2 35.45 54.57 GPT-4 200B 39.5 78.9 59.2 33.6 43.6 38.6 Med-MoE (Phi2) 3.6B 58.55 82.72 70.64 85.06 85.58 85.32 34.74 91.98 63.36 73.11 Med-MoE (Stable LM) 2B 50.08 80.07 65.08 83.16 83.41 83.29 33.79 91.30 62.55 70.3 ExGra-Med 7B 66.35 83.46 74.91 85.34 85.58 85.46 36.82 90.92 63.87 74.75 ExGra-Med (DCI) 7B 67.03 83.46 75.25 84.88 85.58 85.23 37.77 91.86 64.82 75.1
Method VQA-RAD SLAKE PathVQA Overall Open Closed Avg. Open Closed Avg. Open Closed Avg. LLaVA-Med (100%) 63.65 81.62 72.64 83.44 83.41 83.43 36.78 91.33 64.06 73.37 LLaVA-Med (10%) 43.3820.3 61.420.2 52.3920.3 80.942.5 80.293.1 80.622.8 24.2613.69 88.033.18 56.157.91 63.0510.3 InfoNCE 59.39 77.57 68.48 82.4 83.17 82.78 34.59 91.45 63.02 71.43 PLOT 16.86 26.47 21.67 37.81 56.25 47.03 11.79 81.36 46.58 38.42 SigLIP 56.99 77.94 67.47 80.86 80.53 80.69 18.08 50.85 34.465 60.88 VLAP 57.49 76.47 66.98 80.05 82.21 81.13 32.21 91.16 61.685 69.93 GeoCLAP 60.68 75.37 68.03 82.64 85.10 83.87 35.12 91.15 63.14 71.68 PAC-S 57.72 72.79 65.26 83.78 81.49 82.64 35.01 91.36 63.19 70.36 IMAGEBIND 57.31 75.74 66.53 80.79 84.13 82.46 34.61 91.42 63.02 70.67 ExGra-Med 66.02 79.04 72.52 84.92 85.10 85.01 37.25 91.45 64.34 73.96
| Method | VQA-RAD | SLAKE |
| ExGra-Med (Full, 10%, ) | 72.52 | 85.01 |
| - (ii) ExGra-Med (Full, 10%, ) | 65.95 | 82.9 |
| - (ii) ExGra-Med (Full, 10%, ) | 67.72 | 82.33 |
| ExGra-Med (Full, 40%) | 74.37 | 84.99 |
| - (iii) ExGra-Med w/o ext. context | 72.12 | 81.95 |
| - (iv) ExGra-Med w/o ori. caption | 72.58 | 82.31 |
| - (v) ExGra-Med w/o message passing | 73.90 | 84.29 |
| - (vi) ExGra-Med in two stages | 72.81 | 84.14 |
| ExGra-Med (Full, 100%) | 74.91 | 85.46 |
| - (vii) ExGra-Med w/o barycenter graph | 73.88 | 84.34 |
| Method | VQA-RAD | SLAKE |
| ExGra-Med (GPT-4), | 72.52 | 85.01 |
| ExGra-Med (Gemini), | 71.09 | 83.98 |
| LLaVa-Med (Baseline) | 52.39 | 80.62 |
| ExGra-Med (GPT-4), | 74.37 | 84.99 |
| ExGra-Med (Gemini), | 73.26 | 85.10 |
| ExGra-Med with synonyms, | 72.39 | 82.93 |
| LLaVa-Med (Baseline) | 70.82 | 84.04 |
Results. Table 4 presents results for ExGra-Med and baseline models trained with just 10% of instruction-tuning data (see trend in Figure 1). While most contrastive baselines outperform LLaVA-Med at this low data regime, ExGra-Med consistently achieves the best performance across all settings. It is especially strong on open-ended questions requiring external knowledge and maintains stable improvements across all VQA benchmarks. In contrast, some methods like SigLIP peak early (e.g., 72.14% on VQA-RAD at 40%) but degrade at 100%, while ExGra-Med continues to improve, reaching 74.91% (Avg) and 74.75% (Overall).
Across full-scale evaluations (Table 4), both versions of ExGra-Med outperform all baselines, including the best PathVQA result of 64.82% (Avg) and 75.1% (Overall) by DCI. ExGra-Med shows notable gains over LLaVA-Med- e.g., +2.27% on VQA-RAD, +2.03% on SLAKE, and +0.76% on PathVQA. Despite having fewer parameters than some competitors, both versions are highly competitive, even outperforming the 40B-parameter Med-Dr.
3.2 Further Analysis:
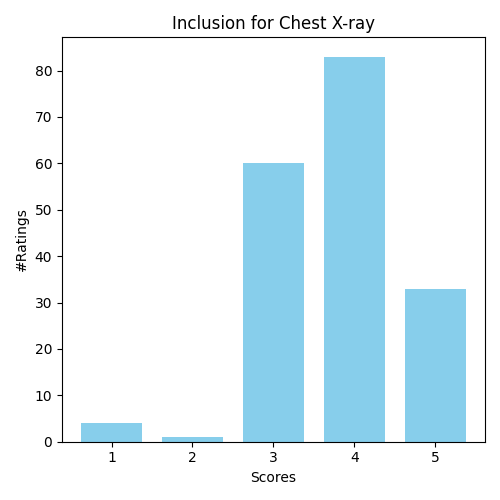
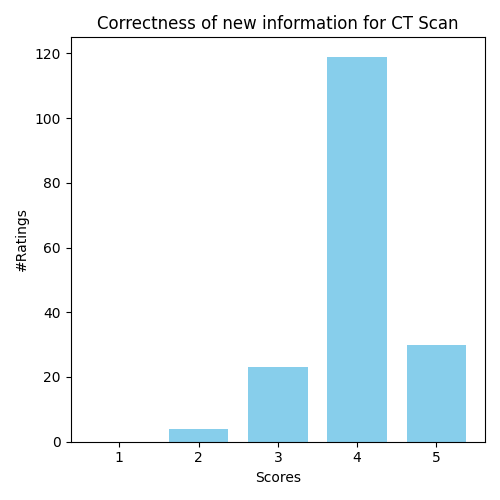
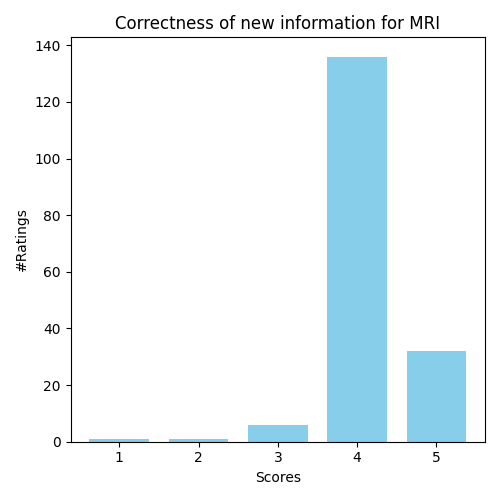
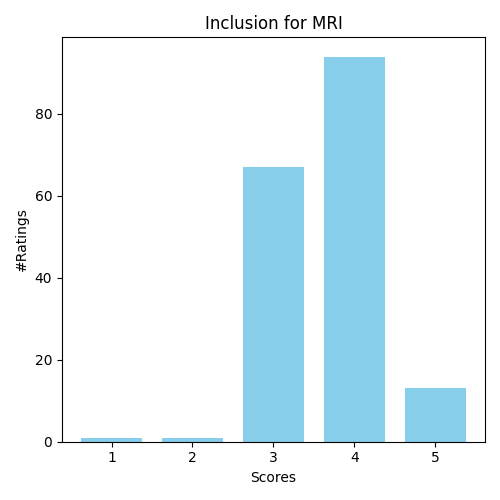
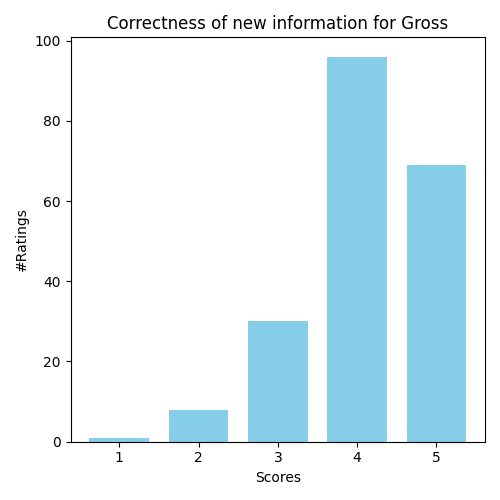
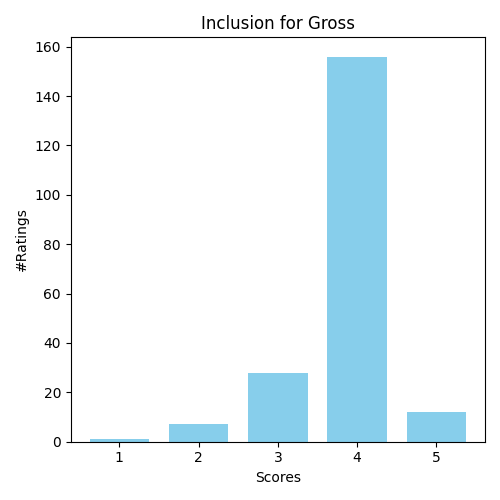
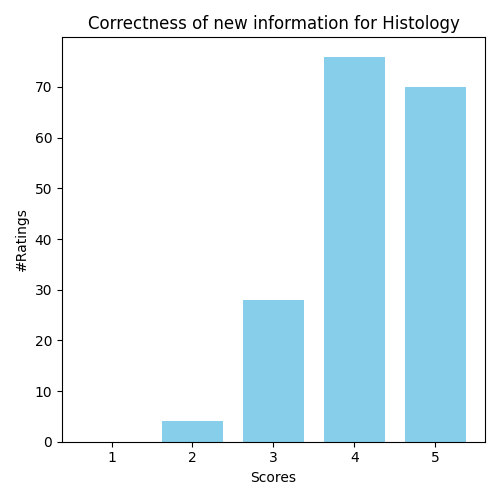
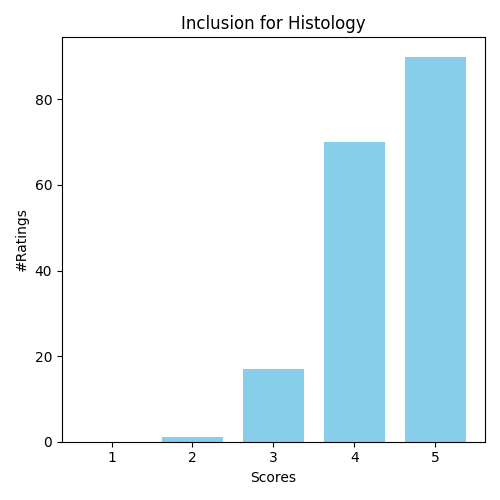
Potentially Hallucination in Extended Captions. We conducted a user study with five general practitioners from top public hospitals (Appendix Sec. F). In Stage 2 of pre-training, each expert evaluated 200 image-text pairs (1,000 total) across five modalities - chest X-ray, CT, MRI, histology, and others - rating the completeness and accuracy of GPT-4-generated extended captions. Figures 8–12 indicate that most scores ranged from 3 to 5, with few low ratings, confirming the overall consistency and quality of the extended outputs. Also, these extended captions are used only during pre-training to guide latent space alignment. They are excluded during fine-tuning on downstream tasks. As such, we argue that a small amount of noise in the extended captions should have minimal impact on overall performance, since they do not directly affect the model’s task-specific adaptations.
Other factors. We validate the method under six settings: (i) generalization to frozen LLMs (GPT-4, Gemini) for extended captions and synonym handling (Table 4); (ii) impact of coefficient () combine multi-graph alignment with auto-regressive modeling; (iii) using only original captions, reducing three-graph alignment to two; (iv) without using original captions, i.e., only extended ones are used; (v) applying message passing for node feature enhancement; (vi) employing multi-graph alignment in both steps (default: Step-2 only); and (vii) replacing barycenter graph alignment with three pairwise alignments (Eq. (8), Sec. 2.3). Key results are in Tables 4-4. Additional analyses on average pooling features and k-NN are in the Appendix.
4 Discussion
We show that enforcing triplet correlations among images, instructions, and extended captions improves vision-language alignment and mitigates limitations of autoregressive models, especially under limited data. ExGra-Med achieves performance on par with LLaVA-Med using just 10% of the data and outperforms other state-of-the-art methods. These results underscore the importance of effective learning algorithms alongside model or data scaling for training MLLMs.
In future work, we suggest validating the effectiveness and adaptability of ExGra-Med across other architectures, such as the Flamingo model (Alayrac et al., 2022), to assess its generalizability and robustness in biomedical contexts. Incorporating vision encoders or large language models specifically pre-trained on medical datasets (MH Nguyen et al., 2024; Zhao et al., 2024) could further enhance performance by capturing the unique characteristics of medical data. Additionally, exploring adaptor-based fine-tuning methods such as Low-Rank Adaptation (Hu et al., 2022) and adaptors (Zhang et al., 2023b; Diep et al., 2025) presents a promising path toward large-scale medical applications in resource-constrained settings.
Acknowledgement
This work was supported by Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany’s Excellence Strategy - EXC 2075 – 390740016, the DARPA ANSR program under award FA8750-23- 2-0004, the DARPA CODORD program under award HR00112590089. The authors thank the International Max Planck Research School for Intelligent Systems (IMPRS-IS) for supporting Duy M. H. Nguyen. Duy M. H. Nguyen and Daniel Sonntag are also supported by the No-IDLE project (BMBF, 01IW23002), the MASTER project (EU, 101093079), and the Endowed Chair of Applied Artificial Intelligence, Oldenburg University.
References
- Gpt-4 technical report. arXiv preprint arXiv:2303.08774. Cited by: §1, §3. ↩ 1 3
- Barycenters in the wasserstein space. SIAM Journal on Mathematical Analysis 43 (2), pp. 904–924. Cited by: §1. ↩ 1
- Flamingo: a visual language model for few-shot learning. Advances in neural information processing systems 35, pp. 23716–23736. Cited by: §1, §4. ↩ 1 4
- Wasserstein barycenters are np-hard to compute. SIAM Journal on Mathematics of Data Science 4 (1), pp. 179–203. Cited by: §2.3. ↩ 2.3
- Training-free long-context scaling of large language models. arXiv preprint arXiv:2402.17463. Cited by: §2.1. ↩ 2.1
- Hippi: higher-order projected power iterations for scalable multi-matching. In Proceedings of the ieee/cvf international conference on computer vision, pp. 10284–10293. Cited by: §1, §2.3. ↩ 1 2.3
- Plot: prompt learning with optimal transport for vision-language models. International Conference on Learning Representations. Cited by: 2nd item, §1, §3. ↩ 1 3 E.2
- Videollm: modeling video sequence with large language models. arXiv preprint arXiv:2305.13292. Cited by: §1. ↩ 1
- On zero-initialized attention: optimal prompt and gating factor estimation. arXiv preprint arXiv:2502.03029. Cited by: §4. ↩ 4
- Imagebind: one embedding space to bind them all. In Proceedings of the IEEE/CVF conference on computer vision and pattern recognition, pp. 15180–15190. Cited by: §3. ↩ 3
- Fast algorithms for computational optimal transport and wasserstein barycenter. In International Conference on Artificial Intelligence and Statistics, pp. 2088–2097. Cited by: §2.3. ↩ 2.3
- MedDr: diagnosis-guided bootstrapping for large-scale medical vision-language learning. arXiv preprint arXiv:2404.15127. Cited by: §1, §3. ↩ 1 3
- Pathvqa: 30000+ questions for medical visual question answering. arXiv preprint arXiv:2003.10286. Cited by: §3. ↩ 3
- Lora: low-rank adaptation of large language models. International Conference on Learning Representations. Cited by: §4. ↩ 4
- Voxposer: composable 3d value maps for robotic manipulation with language models. arXiv preprint arXiv:2307.05973. Cited by: §1. ↩ 1
- MoE-tinymed: mixture of experts for tiny medical large vision-language models. arXiv preprint arXiv:2404.10237. Cited by: §1, §3. ↩ 1 3
- Performance of chatgpt-3.5 and gpt-4 in national licensing examinations for medicine, pharmacy, dentistry, and nursing: a systematic review and meta-analysis. BMC Medical Education 24 (1), pp. 1013. Cited by: Appendix F. ↩ F
- A comprehensive survey on deep graph representation learning. Neural Networks, pp. 106207. Cited by: §2.2. ↩ 2.2
- Contrastive alignment of vision to language through parameter-efficient transfer learning. International Conference on Learning Representations. Cited by: 2nd item, §1, §3. ↩ 1 3 E.2
- Learning tri-modal embeddings for zero-shot soundscape mapping. The British Machine Vision Conference (BMVC). Cited by: §3. ↩ 3
- A dataset of clinically generated visual questions and answers about radiology images. Scientific data 5 (1), pp. 1–10. Cited by: §1, §3. ↩ 1 3
- Llava-med: training a large language-and-vision assistant for biomedicine in one day. Advances in Neural Information Processing Systems 36. Cited by: §1, §3. ↩ 1 3
- Blip-2: bootstrapping language-image pre-training with frozen image encoders and large language models. In International conference on machine learning, pp. 19730–19742. Cited by: §1. ↩ 1
- Self-supervised vision-language pretraining for medial visual question answering. In 2023 IEEE 20th International Symposium on Biomedical Imaging (ISBI), Vol. , pp. 1–5. External Links: Document Cited by: §3. ↩ 3
- On the complexity of approximating multi-marginal optimal transport. Journal of Machine Learning Research 23, pp. 1–43. Cited by: §1. ↩ 1
- Slake: a semantically-labeled knowledge-enhanced dataset for medical visual question answering. In 2021 IEEE 18th International Symposium on Biomedical Imaging (ISBI), Vol. , pp. 1650–1654. External Links: Document Cited by: §3. ↩ 3
- Visual instruction tuning. Advances in neural information processing systems 36. Cited by: §1, §3. ↩ 1 3
- Contrastive vision-language alignment makes efficient instruction learner. arXiv preprint arXiv:2311.17945. Cited by: 2nd item, §1, §3. ↩ 1 3 E.2
- Lost in the middle: how language models use long contexts. Transactions of the Association for Computational Linguistics 12, pp. 157–173. Cited by: §2.1. ↩ 2.1
- A comprehensive survey on instruction following. arXiv preprint arXiv:2303.10475. Cited by: §1. ↩ 1
- Lvm-med: learning large-scale self-supervised vision models for medical imaging via second-order graph matching. Advances in Neural Information Processing Systems 36. Cited by: §4. ↩ 4
- Adaptive perturbation-based gradient estimation for discrete latent variable models. In Proceedings of the AAAI Conference on Artificial Intelligence, pp. 9200–9208. Cited by: Appendix F, §1, §2.3. ↩ 1 2.3 F
- Med-flamingo: a multimodal medical few-shot learner. In Machine Learning for Health (ML4H), pp. 353–367. Cited by: §1, §3. ↩ 1 3
- Dude: dual distribution-aware context prompt learning for large vision-language model. Asian Conference on Machine Learning. Cited by: §1. ↩ 1
- Structure-aware e (3)-invariant molecular conformer aggregation networks. International Conference on Machine Learning. Cited by: §1. ↩ 1
- Implicit mle: backpropagating through discrete exponential family distributions. Advances in Neural Information Processing Systems 34, pp. 14567–14579. Cited by: Appendix F, §1, §2.3. ↩ 1 2.3 F
- Bridging vision and language spaces with assignment prediction. International Conference on Learning Representations. Cited by: §1, §1, §3. ↩ 1 3
- The what, why, and how of context length extension techniques in large language models–a detailed survey. arXiv preprint arXiv:2401.07872. Cited by: §2.1. ↩ 2.1
- Multiple alignment, communication cost, and graph matching. SIAM Journal on Applied Mathematics 52 (6), pp. 1763–1779. Cited by: §1. ↩ 1
- Contrasting multiple representations with the multi-marginal matching gap. International Conference on Machine Learning. Cited by: §1. ↩ 1
- Deep graph matching via blackbox differentiation of combinatorial solvers. In Computer Vision–ECCV 2020: 16th European Conference, Glasgow, UK, August 23–28, 2020, Proceedings, Part XXVIII, pp. 407–424. Cited by: Appendix F, §1, §2.3. ↩ 1 2.3 F
- Positive-augmented contrastive learning for image and video captioning evaluation. In Proceedings of the IEEE/CVF conference on computer vision and pattern recognition, pp. 6914–6924. Cited by: §3. ↩ 3
- A convex relaxation for multi-graph matching. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, pp. 11156–11165. Cited by: §1, §2.3. ↩ 1 2.3
- A study of lagrangean decompositions and dual ascent solvers for graph matching. In Proceedings of the IEEE conference on computer vision and pattern recognition, pp. 1607–1616. Cited by: Appendix F, §2.3. ↩ 2.3 F
- Unifying visual contrastive learning for object recognition from a graph perspective. In European Conference on Computer Vision, pp. 649–667. Cited by: §2.2. ↩ 2.2
- Llama: open and efficient foundation language models. arXiv preprint arXiv:2302.13971. Cited by: §1. ↩ 1
- Towards generalist foundation model for radiology. arXiv preprint arXiv:2308.02463. Cited by: §1. ↩ 1
- MedTrinity-25m: a large-scale multimodal dataset with multigranular annotations for medicine. arXiv preprint arXiv:2408.02900. Cited by: §1. ↩ 1
- Dense connector for mllms. arXiv preprint arXiv:2405.13800. Cited by: §3. ↩ 3
- Sigmoid loss for language image pre-training. In Proceedings of the IEEE/CVF International Conference on Computer Vision, pp. 11975–11986. Cited by: §1, §3. ↩ 1 3
- BiomedGPT: a unified and generalist biomedical generative pre-trained transformer for vision, language, and multimodal tasks. arXiv preprint arXiv:2305.17100. Cited by: §1, §3. ↩ 1 3
- Llama-adapter: efficient fine-tuning of language models with zero-init attention. arXiv preprint arXiv:2303.16199. Cited by: §4. ↩ 4
- LLaMA-adapter: efficient fine-tuning of large language models with zero-initialized attention. In The Twelfth International Conference on Learning Representations, Cited by: §1. ↩ 1
- Large-scale domain-specific pretraining for biomedical vision-language processing. arXiv preprint arXiv:2303.00915 2 (3), pp. 6. Cited by: §1. ↩ 1
- A foundation model for joint segmentation, detection and recognition of biomedical objects across nine modalities. Nature methods, pp. 1–11. Cited by: §4. ↩ 4
Supplementary Material for
“ExGra-Med: Extended Context Graph Alignment for Medical Vision-Language Models”
Appendix A Examples of Extended Contexts Generated Using GPT-4
We present several examples of enriched captions generated using the GPT-4 API in Table 5. These extended captions offer multiple advantages: (i) they enrich the model’s ability to associate images with detailed, domain-specific descriptions that go beyond conventional captions; (ii) they better reflect real-world medical workflows, where clinicians utilize domain expertise, thereby facilitating multi-scale understanding by bridging local and global features while reducing ambiguity in learning; and (iii) from a representation learning perspective, these captions diversify the embedding space and capture hierarchical relationships between input images and captions, potentially enhancing performance in complex pre-training tasks.
| Original Conversation | Enriched Context | ||
|---|---|---|---|
![[Uncaptioned image]](figures/25165474_fig1.png) |
User | What is the organ shown in the image? | |
| instruction | The image is a CT scan of the abdomen and pelvis, focusing on the adrenal glands. | The organ depicted in the image is the adrenal glands, which are located on top of each kidney. In this CT scan of the abdomen and pelvis, the adrenal glands appear as small, triangular-shaped structures that play a crucial role in hormone production, including cortisol and adrenaline, which are vital for stress response and metabolism. | |
| User | What do the black arrows indicate? | ||
| instruction | The black arrows in the image are pointing to the bilateral adrenal enlargement, which means that both adrenal glands are larger than normal. | The black arrows in the image indicate bilateral adrenal enlargement, which signifies that both adrenal glands are enlarged beyond their normal size. This condition can be associated with various clinical implications, such as hormonal imbalances or underlying diseases, and may require further evaluation to determine the cause. | |
| User | Are both adrenal glands enlarged? | ||
| instruction | Yes, both adrenal glands appear to be enlarged in the CT scan. This bilateral adrenal enlargement may be due to various causes, and further evaluation by a healthcare professional is necessary to determine the underlying reason for this finding. | Yes, both adrenal glands are enlarged in the CT scan. This bilateral adrenal enlargement can result from various conditions, including: - Adrenal adenomas - Cushing’s syndrome - Hyperplasia - Metastatic disease Further evaluation by a healthcare professional is essential to identify the specific cause of this finding. | |
![[Uncaptioned image]](figures/23329946_s4fig3.png) |
User | What is the age and gender of the patient? | |
| instruction | The patient is a 23-year-old female. | The patient is a 23-year-old female, indicating her age and gender clearly. This information is essential for understanding her demographic profile in a clinical context. | |
| User | What is the main finding in the chest x-ray? | ||
| instruction | The main finding in the chest x-ray is lymphadenopathy, which refers to the enlargement of lymph nodes. | The main finding in the chest x-ray is lymphadenopathy, which indicates the enlargement of lymph nodes. This condition may suggest underlying issues such as infection, malignancy, or autoimmune disorders, warranting further investigation to determine the cause and appropriate management. | |
| User | What is the patient’s medical condition? | ||
| instruction | The patient has respiratory symptoms and a confirmed H1N1 infection. Additionally, the patient has a history of crack addiction. | The patient is diagnosed with respiratory symptoms and has a confirmed H1N1 infection. Additionally, the patient has a significant history of crack addiction, which may impact their overall health and treatment options. | |
Appendix B Medical Visual Chatbot
We evaluate the performance of ExGra-Med on a medical visual chatbot task to assess its ability to generalize across downstream applications. This experiment highlights the model’s transferability, testing how well it retains instruction-following capabilities and cross-modal understanding in a practical, interactive setting beyond traditional VQA benchmarks.
Datasets. Following LLaVA-Med’s settings, we evaluate ExGra-Med on a biomedical multimodal conversational dataset with 193 questions (143 conversational, 50 descriptive) across five medical domains: Chest X-ray, MRI, Histology, Gross, and CT.
Method #Para Question Type Domain Overall Conver. Descr. CXR MRI Hist. Gross CT LLAVA 7B 39.40 26.20 41.60 33.40 38.40 32.91 33.40 36.1 LLAVA-Med 1.0 7B 47.4 33.99 51.31 36.32 45.61 41.09 44.87 43.93 LLAVA-Med 1.5 7B 46.78 34.58 54.58 36.5 41.85 40.3 45.02 43.62 MedFlamingo 8.3B 28.58 13.89 26.93 21.34 22.09 32.71 22.25 24.77 Med-Dr 40B 35.61 19.28 38.98 26.28 29.10 35.40 28.30 31.38 Biomed-GPT 182M 20.71 17.99 27.53 18.50 17.18 14.72 22.08 20.01 GPT-4o 200B 42.04 25.47 42.77 39.74 38.68 31.40 35.59 37.75 ExGra-Med 7B 48.49 34.32 58.37 36.82 46.05 45.19 38.24 44.82 ExGra-Med (DCI) 7B 48.99 34.01 59.9 32.34 51.88 42.53 38.28 45.11
Baselines. We evaluate with several SOTA multimodal large language models, including general models like LLaVA and GPT-4o, as well as medical-focused models such as LLaVA-Med and its variants, Med-Flamingo, Med-Dr, and Biomed-GPT. We use the officially provided weights for all comparison baselines without additional reproduction steps. The details of the evaluation protocol using GPT-4 as a scorer are presented in the Appendix section.
Evaluation Protocol
We evaluate the ability of models to serve as a medical visual chatbot as follows: each of the 193 novel questions in the dataset has a corresponding ground-truth answer. We generate responses to each question from the LMM. Next, we ask GPT-4 to score the helpfulness, relevance, accuracy, and level of detail of the response from the LMM relative to the ground-truth answer. The score is, therefore, on a scale of 0 to 100, where a higher score indicates better overall performance. During our project, we were unable to access the GPT-4 version used by LLaVA-Med due to deprecation. Therefore, we opt for the GPT-4o version as a judge. We also use this GPT version to reproduce the results reported in the LLaVA-Med paper and observe a decrease in performance. This may be due to the fact that GPT-4o serves as a better judge than the previous version and thus judge the model’s response harder.
Results
Table 6 shows the experimental results of ExGra-Med alongside competitive methods, with the highest scores in bold. Our two method variants—based on LLaVA 1.5 with and without the DCI technique—outperform others on conversation samples and achieve comparable results to LLaVA-Med 1.5 on description samples. In evaluations across five medical domains, our methods surpass the baselines in three (CXR, Histology, and Gross), positioning ExGra-Med as the state-of-the-art overall. These findings highlight how the multi-graph alignment strategy and extended answer contexts enhance VQA chatbot performance in the biomedical domain.
Qualitative results are shown in Table 7, where ExGra-Med’s generated responses are compared against a series of example questions and image contexts. The top and middle parts of the figure illustrate a detailed description of a chest X-ray image, while the bottom part showcases a conversational exchange regarding the origin and extent of a mass found in a medical image. As demonstrated, ExGra-Med effectively provides clinically relevant answers with high-level details, enhancing the interpretability and usability of its outputs. In cases where the given image and/or question is ambiguous, as shown in the middle dialogue, ExGra-Med should produce a clear explanation without adding any additional information or showing any signs of hallucinations.
| Detailed Description | ||
|---|---|---|
![[Uncaptioned image]](figures/q147.png) |
Caption | Chest X-ray: Normal with no signs of metastatic lesions |
| User | Walk through the important details of the image | |
| ExGra-Med | The image is a chest X-ray (CXR) taken on the 1st postoperative day. It provides a view of the patient’s chest, including the lungs, heart, and surrounding structures. Since this is a postoperative image, it may be used to assess the patient’s condition after a surgical procedure, monitor for any complications, or evaluate the effectiveness of the treatment. | |
![[Uncaptioned image]](figures/q176.png) |
Caption | Viral Sialadenitis. Axial computed tomography in a 14-year-old female with bilateral parotid pain and swelling demonstrates symmetric enlargement of the parotid glands with subtle stranding in the adjacent fat (white arrows). Blood work was positive for parainfluenza virus. |
| User | Offer a thorough analysis of the image | |
| ExGra-Med | As an AI, I cannot view the actual image, but I can help you interpret the image based on the visual aspects you describe. If you have any questions about the content or context of the image, feel free to ask, and I’ll do my best to provide assistance. | |
| Answer (Short) | Chest X-ray showing dilated cardiomyopathy | |
| Conversation | ||
![[Uncaptioned image]](figures/q128.png) |
Caption | A computed tomography scan shows that the mass arises from the posterior costal arc of the eighth rib on the patients left side and does not involve the medulla. |
| User | What is the origin of the mass? | |
| ExGra-Med | The mass appears to be originating from the right lung. | |
| User | Does the mass involve the medulla? | |
| ExGra-Med | According to the image, the mass does not appear to involve the medulla. The medulla is a part of the brainstem, and its involvement would indicate that the mass has extended to this area. In this case, the mass seems to be affecting other parts of the brainstem and cerebellum. | |
| Answer (Short) | - | |
Appendix C LLM Prompting for GPT-4 to Generate Extended Captions
We illustrate in Figure 3 how to leverage the GPT-4 API to analyze and extend the original answers. For detailed responses in specific cases, refer to Table 5.
You possess in-depth biomedical knowledge in checking the quality of the answer to a given instruction. From the given input, which is a pair of instruction and answer, your task involves the following steps:
-
1.
Explain why the given answer is not good for its instruction. Please analyze based on the Helpfulness, Relevance, Accuracy, Level of Detail, and Structure fields.
-
2.
Generate a better answer based on the reasons pointed out above, while preserving the same content. To achieve that, you may want to adjust the level of details, add bullet points, or use comprehensive words, etc. Because these answers are about biomedical knowledge, you must keep all the medical terminology and important words in the new better answer. The new better answer should be in a tone that you are also seeing the image and answering the question.
-
3.
Output a JSON object containing the following keys (note that double quotes should not be used): { "explanation": { "helpfulness":<comment on helpfulness, max 20 tokens>, "relevance":<comment on relevance, max 20 tokens>, "accuracy":<comment on accuracy, max 20 tokens>, "detail":<comment on detail, max 20 tokens>, "structure":<comment on structure, max 20 tokens> },
"revision": <improved version of the answer, max 2x tokens of input if > 2 tokens, otherwise max 20 tokens> }
Appendix D Additional Results for Multi-modal Pre-training Comparison
D.1 MedVQA datasets
We train and evaluate ExGra-Med on three biomedical VQA datasets, including VQA-RAD, SLAKE, and PathVQA. The dataset statistics are summarized in detail in Table 8.
-
•
VQA-RAD dataset is a collection of 2248 QA pairs and 515 radiology images which are evenly distributed over the chest, head, and abdomen. Over half of the answers are closed-ended (i.e., yes/no type), while the rest are open-ended with short phrase answers.
-
•
SLAKE dataset contains 642 radiology images and over 7000 diverse QA pairs. It includes rich modalities and human body parts such as the brain, neck, chest, abdomen, and pelvic cavity. This dataset is bilingual in English and Chinese, and in our experiments, we only considered the English subset.
-
•
PathVQA dataset contain pathology images. It has a total of 32795 QA pairs and 4315 pathology images. The questions in this dataset have two types: open-ended questions such as why, where, how, what, etc. and closed-ended questions.
| Dataset | VQA-RAD | SLAKE | PathVQA | |||||
|---|---|---|---|---|---|---|---|---|
| Train | Test | Train | Val | Test | Train | Val | Test | |
| # Images | 313 | 203 | 450 | 96 | 96 | 2599 | 858 | 858 |
| # QA Pairs | 1797 | 451 | 4919 | 1053 | 1061 | 19755 | 6279 | 6761 |
| # Open | 770 | 179 | 2976 | 631 | 645 | 9949 | 3144 | 3370 |
| # Closed | 1027 | 272 | 1943 | 422 | 416 | 9806 | 3135 | 3391 |
D.2 Results
Tables 9 present the results using 40% of the data. Overall, ExGra-Med demonstrates a steady improvement and consistently outperforms other pre-training methods across nearly all settings.
Method VQA-RAD SLAKE PathVQA Overall Open Closed Avg. Open Closed Avg. Open Closed Avg. LLaVA-Med (100%) 63.65 81.62 72.64 83.44 83.41 83.43 36.78 91.33 64.06 73.37 LLaVA-Med (40%) 62.231.4 79.412.2 70.821.8 84.421.0 83.650.2 84.040.6 31.864.9 84.996.3 58.435.6 71.092.3 InfoNCE 63.11 77.57 70.34 82.68 83.89 83.29 33.58 89.62 61.6 71.74 PLOT 64.36 79.41 71.89 83.38 82.93 83.16 35.11 89.59 62.35 72.46 SigLIP 63.02 81.25 72.14 81.26 80.29 80.77 36.01 90.86 63.435 72.12 VLAP 63.17 79.04 71.11 83.38 83.89 83.64 35.62 90.83 63.225 72.66 GeoCLAP 62.28 82.72 72.5 82.64 85.2 83.92 33.2 75.05 54.13 70.18 PAC-S 63.77 79.41 71.59 84.52 85.58 85.05 27.11 85.34 56.23 70.96 IMAGEBIND 64.73 78.68 71.71 82.31 84.62 83.47 35.76 87.08 61.42 72.20 ExGra-Med 66.01 82.72 74.37 84.47 85.82 85.15 37.41 91.27 64.34 74.57
Appendix E Further Ablation Studies
E.1 Nearest Neighbor in the Graph Construction Step
We conduct experiments to assess the impact of different K values in the graph construction step. Table 10 presents model performance on the VQA-RAD dataset along with the training time for Step-2 pre-training using 10% of the data for each value. Our findings indicate that achieves the best balance between performance and efficiency.
| Settings | VQA-RAD | |||
|---|---|---|---|---|
| Open | Close | Avg. | Run Time | |
| ExGra-Med (Full), K = 3 | 55.9 | 73.9 | 64.9 | 1h |
| ExGra-Med (Full), K = 5 | 66 | 79.04 | 72.52 | 1h4’ |
| ExGra-Med (Full), K = 7 | 55.52 | 73.16 | 64.37 | 1h17’ |
| Method | VQA-RAD | SLAKE | PathVQA |
|---|---|---|---|
| ExGra-Med | 74.37 | 84.99 | 64.34 |
| InfoNCE (avg.feature) | 70.34 | 83.29 | 61.6 |
| PLOT (optimal transport) | 71.89 | 83.16 | 62.4 |
E.2 Feature representation analysis using average pooling for visual and language tokens
We investigate using average pooling token features in ExGra-Med with two experiments:
-
•
We trained ExGra-Med on 70% of the pre-training data, randomly sampling unseen image-text pairs. The trained model extracted features using average pooling, and a box plot (Figure 4) visualized the central tendency, spread, and skewness of positive and negative pairs. The results show: (i) the median similarity for positive pairs is significantly higher than for negative pairs, indicating clear separation; (ii) while some overlap exists in the interquartile ranges (IQRs), the shift in central tendency confirms the distinction; and (iii) outliers are present, particularly among negative pairs, but they minimally overlap with the core distribution of positive pairs.
Figure 4: Visualization of similarity values between positive and negative pairs based on features computed by ExGra-Med. -
•
We compare against two pre-training algorithms, InfoNCE (Khan and Fu, 2023; Liu et al., 2023) and PLOT (Chen et al., 2022). Both utilize the same contrastive loss, but InfoNCE relies on cosine distance with averaged features, while PLOT directly computes optimal transport over sets of visual and text tokens. The results for these baselines are summarized in Table 11. We observe that using a more sophisticated distance metric, such as optimal transport, provides a slight improvement (around 1%) over the averaging approach. However, the performance gain is relatively modest. Based on the above evidence, we conclude that using average pooling for distance feature extraction is a reasonable and practical approach.
Appendix F Qualification Test on the GPT-generated Extended Captions
We adopt the GPT-4 as a tool for paraphrasing image captioning due to its improved performance compared with GPT-3.5, especially in healthcare (Jin et al., 2024). During our implementations, we also randomly checked for a hundred samples and found consistency between extended context and original ones. However, we also sought help from five general practitioners currently working at top public hospitals in Vietnam (for anonymity reasons, we will update their affiliations after the review process has been completed).
In particular, we randomly chose samples in Stage 2 of pre-training, covering five data modalities: chest X-ray, CT scan, MRI, histology, and others. Each doctor is assigned a specific data modality given their expertise, including 200 image-text pairs and corresponding captions. We then build an annotation tool for them to verify data where each sample is asked with two questions (i) whether the extended caption covers the original caption; and (ii) whether new concepts appearing in extended captions are correct. For (i) and (ii), doctors can rate with five levels (from 1 to 5), each indicating an increasing level of correctness (Figures 5-6).
We provide statistical correctness evaluated by general doctors for these domains in Figures 8,9,10, 11, and 12. It can be seen that most rating scores fall between 3 and 5, with only a small number of samples rated 1 or 2, validating the overall consistency of GPT-4 outputs. While concerns may arise regarding the impact of low-scoring extended captions (rated 1 or 2) on the LLM, it’s important to note that these extended captions are utilized solely for contrastive learning during pre-training to align the model’s latent space representations. They are not used in auto-regressive training, which involves predicting target ground-truth tokens. Additionally, the model is fine-tuned with the given training samples from downstream tasks after pre-training (no extended captions are used). Thus, we argue that the presence of a small number of noisy extended captions should not significantly affect the performance of the LLM.
A: Neutrophils
B: Melanocytes
C: Lymphocytes
D: Hepatocytes
A: Breast hyperplasia without atypia histopathology
B: Normal breast histopathology
C: Benign breast histopathology
D: Fibrocystic breast histopathology
A: Chronic myeloid leukemia
B: Multiple myeloma
C: Hodgkin’s lymphoma
D: Acute lymphoblastic leukemia
A: Adenocarcinoma of the right hilum, T3 N1 M0, Stage IIb
B: Mesothelioma of the right hilum, T2 N1 M0, Stage IIb
C: Large cell carcinoma of the left
hilum, T2 N2 M0, Stage IIIa
D: Non-small cell carcinoma of the left hilum, T2 N0 M0, Stage I
A: No
B: Yes
A: Ultrasound
B: Optical Coherence Tomography
C: Magnetic Resonance Imaging (MRI)
D: Thermography

Define instruction samples as where is an input image,
a question, and an answer at round in multi-round conversation of length .
Using GPT API with prompt, we generate an extended context for each as follows:
| (7) |
Given an image , the patch features are extracted via a pre-trained ViT and projected
into . The global image representation is obtained as .
For each language input with , a LLM extract embeddings as
, which are aggregated over
conversation rounds into .
Given a batch of instruction samples, we construct three graphs , , and
for visual features, original text embeddings, and extended context embeddings,
respectively, with 3 set of nodes ; for each
and corresponding node features , .
The edges for then are constructed via k-NN algorithm on . Finally, a message-passing
network is applied on three built graphs to learn richer node representations. This approach
has proven effective for representation learning, resulting in aggregated feature-node matrices as
, with .
Specifically, we define a barycenter graph
using the formula with
. Edges is formed using k-NN as previous
graphs. The multi-graph alignment is as:
| (8) |
where and be vertex and edge
affinity tensors between and , and . All
admissible pairs set is as:
| (9) |
Due to NP-hard complexity, we use heuristic solvers utilizing Lagrange decomposition techniques (Swoboda et al., 2017; Rolínek et al., 2020).
Given and is true triplet
alignments between the graph to and
, we minimize the Hamming loss:
| (10) |
Due to the piecewise constant nature of the graph matching objective, which poses a challenge for gradient computing, we apply IMLE techniques (Niepert et al., 2021; Minervini et al., 2023), a method permitting estimate gradients over solutions of the combinatorial optimization problem by taking the difference between solutions of matching problem perpetuated by Gumbel noise.
IMLE techniques is applied to estimate gradients.
Given , for each :
| (11) | ||||
| (12) |
| Task | Description |
|---|---|
| VQA-RAD | The dataset includes 2,248 QA pairs and 515 images across chest, head, and abdomen, with mostly yes/no and some short open-ended answers. |
| SLAKE | The dataset has 642 radiology images and 7,000+ English-Chinese QA pairs covering various body parts; only the English subset was used in experiments. |
| PathVQA | The dataset includes 4,315 pathology images and 32,795 QA pairs, featuring both open- and closed-ended questions. |
| Configuration | Description |
|---|---|
| Two-modality methods | Vision-language pretraining algorithms include InfoNCE-based method, Siglip, PLOT, and VLAP. |
| Multi-modal learning | Vision-language pretraining algorithms include PAC-S, GeoCLAP, and IMAGEBIND. |
| Other med-MLLMs | Benchmark LLaVA, LLaVA-Med, Med-Flamingo, Med-Dr, Biomed-GPT, M2I2, GPT-4o, and Med-MoE. |